Story submitted - 2020
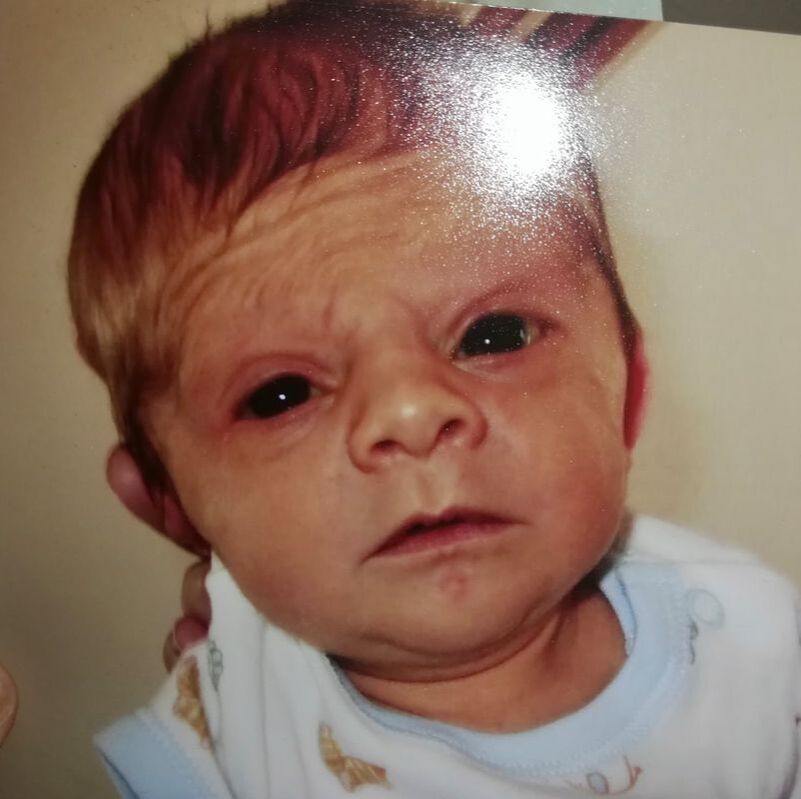
Charlie was born in March of 2007 weighting 6lb 10oz (3.08kg), very small compared to his other siblings, who were up to 8lbs 10oz 3.9kg). It was a normal pregnancy except that he was 2 weeks overdue, making the small size even more surprising. The paediatrician on birth described him as having coarse features. He also had an issue with his eye (eyelid very droopy) and was diagnosed as having an undescended testicle.
The paediatrician described Charlie as having ‘coarse features’ but did not indicate anything further that was of concern in relation to this, but later it came out that he thought that this was a sign to him that there was something genetic going on.
On discharge, although Charlie fed well, he was not gaining weight and was described as having a ‘failure to thrive’ – he was not discharged to the general practitioner as is normal for routine follow up checks, but instead we had to go to the hospital for his follow up checks for a full year. Charlie did not meet any of the normal milestones during that first year. He could not roll over or sit up and needed physiotherapy to help him learn those movements. A dietician prescribed PediaSure to help him put on weight, but he remained way below any weight or height chart.
Charlie was born in March of 2007 weighting 6lb 10oz (3.08kg), very small compared to his other siblings, who were up to 8lbs 10oz 3.9kg). It was a normal pregnancy except that he was 2 weeks overdue, making the small size even more surprising. The paediatrician on birth described him as having coarse features. He also had an issue with his eye (eyelid very droopy) and was diagnosed as having an undescended testicle.
The paediatrician described Charlie as having ‘coarse features’ but did not indicate anything further that was of concern in relation to this, but later it came out that he thought that this was a sign to him that there was something genetic going on.
On discharge, although Charlie fed well, he was not gaining weight and was described as having a ‘failure to thrive’ – he was not discharged to the general practitioner as is normal for routine follow up checks, but instead we had to go to the hospital for his follow up checks for a full year. Charlie did not meet any of the normal milestones during that first year. He could not roll over or sit up and needed physiotherapy to help him learn those movements. A dietician prescribed PediaSure to help him put on weight, but he remained way below any weight or height chart.
|

|

|
At age one they admitted him for a week and began a series of tests on his heart, lungs, gastrointestinal system, all were fine. They began genetic tests – he was tested for Williams syndrome and others, all negative, so they eventually sent his sample for full genetic analysis. We noticed seizure activity from about age 1 year (myoclonic jerks about 20 times/day) and he was diagnosed with epilepsy aged about 14 months, when referred to a consultant and had an EEG. He was treated with Epilim but had status epilepticus around 1.5 years, that did not resolve with emergency medication. He ended up in ICU and on a ventilator but recovered after a few days.
In 2009 and he was found to have a large deletion in the SMARCA2 gene. We were both tested and did not have the deletion, so it was new in him. At that point there was no connection made to NCBRS and we were told that he was the only child registered with the deletion (though this was actually not the case it seems based on other cases we know of now). As such there was no network of support. By age 2 he suffered from atopic dermatitis. He was also admitted that year for an operation for the undescended testicle and this was repaired, but later the other testicle disappeared into the abdomen and he had another procedure to bring that down. On a yearly basis in winter through childhood to now he was prone to conjunctivitis. He finally started to walk age 2. He had very delayed speech, first words maybe aged 3.5-4 years. He initially started to learn sign language to communicate but now speaks fluently, however repeats the same things very often.
He was registered with the local disability service and had home visits with OT and speech activities from about age 2 and went to a regular preschool from age 4, with the support of a special needs assistant. He moved to a mainstream school when he was 6. He had a part time support to assist him, less than 50% of the time. It worked ok for a while and Charlie stayed for 4 years in mainstream, but at that point it was clear he needed additional support and the gap was widening between him and his classmates. He could not write or read, was not consistently getting colours right or counting after 4 years in school (he now recognises certain words but does not understand phonics). Through clinical psychologist assessment he was diagnosed as having a moderate to severe intellectual disability. The teachers agreed that what he needed was a school that looked after him in a more practical life skills approach rather than an academic one and he moved to a special school when he was 10. Initially this was difficult as none of his class mates had been to mainstream and there were behavioural issues in the class, but this settled after the first year.
In 2009 and he was found to have a large deletion in the SMARCA2 gene. We were both tested and did not have the deletion, so it was new in him. At that point there was no connection made to NCBRS and we were told that he was the only child registered with the deletion (though this was actually not the case it seems based on other cases we know of now). As such there was no network of support. By age 2 he suffered from atopic dermatitis. He was also admitted that year for an operation for the undescended testicle and this was repaired, but later the other testicle disappeared into the abdomen and he had another procedure to bring that down. On a yearly basis in winter through childhood to now he was prone to conjunctivitis. He finally started to walk age 2. He had very delayed speech, first words maybe aged 3.5-4 years. He initially started to learn sign language to communicate but now speaks fluently, however repeats the same things very often.
He was registered with the local disability service and had home visits with OT and speech activities from about age 2 and went to a regular preschool from age 4, with the support of a special needs assistant. He moved to a mainstream school when he was 6. He had a part time support to assist him, less than 50% of the time. It worked ok for a while and Charlie stayed for 4 years in mainstream, but at that point it was clear he needed additional support and the gap was widening between him and his classmates. He could not write or read, was not consistently getting colours right or counting after 4 years in school (he now recognises certain words but does not understand phonics). Through clinical psychologist assessment he was diagnosed as having a moderate to severe intellectual disability. The teachers agreed that what he needed was a school that looked after him in a more practical life skills approach rather than an academic one and he moved to a special school when he was 10. Initially this was difficult as none of his class mates had been to mainstream and there were behavioural issues in the class, but this settled after the first year.
|

|

|
Charlie has good gross motor skills and loves to swim and play and climb in the playground, but still has issues with fine motor skills. He can eat independently, although knows what he likes to eat – more limited food items than the rest of the family. He can follow instruction. He has some autistic type tendencies in terms of behaviour and tends to obsess about certain things – for example car types, supermarket names, he loves logos and slogans which he will repeat over and over. If he has a plan in his head it is hard to divert him from that and that can sometimes lead to behavioural issues, but these resolve quickly. His attention span is very low.
Saying that social skills are Charlie’s strength. He is a very friendly, sociable child who loves everyone and is loved by all in return. Everyone knows him in the area. He loves music and dance and has great rhythm. He loves going to the park, going out for drives, on the train or bus and particularly loves going to the supermarket where he insists on tidying up all baskets and trolleys. He wants to work in a supermarket when he grows up.
He seems to live from event to event. Once Christmas is over he talks about his birthday. Then Easter, then holidays, then Halloween etc. he has no concept of time so talks about things that are months away as if they are tomorrow!
Charlie continues to have seizures, but generally only when he comes down with some sort of infection or is very tired. His seizures were myoclonic but now tend to be absence seizures. This is more dangerous for him in some ways as he will try to get up and has fallen and hit his head twice resulting in a trip to A&E (most seizures are at night).
Charlie had hormone level testing when he was around 5-6 due to short stature, but all was normal. Charlie is toilet trained maybe aged 6-7 but still wears a pull up at night. He likes to help with activities around the house sweeping and Hoovering and putting on the washing (sometimes puts on the machine while empty!) Charlie sleeps well – when younger he used to come into our bed around 5-6 am but would go straight back asleep again. It worked well as early morning was when he had seizures so we could keep an eye on him.
Saying that social skills are Charlie’s strength. He is a very friendly, sociable child who loves everyone and is loved by all in return. Everyone knows him in the area. He loves music and dance and has great rhythm. He loves going to the park, going out for drives, on the train or bus and particularly loves going to the supermarket where he insists on tidying up all baskets and trolleys. He wants to work in a supermarket when he grows up.
He seems to live from event to event. Once Christmas is over he talks about his birthday. Then Easter, then holidays, then Halloween etc. he has no concept of time so talks about things that are months away as if they are tomorrow!
Charlie continues to have seizures, but generally only when he comes down with some sort of infection or is very tired. His seizures were myoclonic but now tend to be absence seizures. This is more dangerous for him in some ways as he will try to get up and has fallen and hit his head twice resulting in a trip to A&E (most seizures are at night).
Charlie had hormone level testing when he was around 5-6 due to short stature, but all was normal. Charlie is toilet trained maybe aged 6-7 but still wears a pull up at night. He likes to help with activities around the house sweeping and Hoovering and putting on the washing (sometimes puts on the machine while empty!) Charlie sleeps well – when younger he used to come into our bed around 5-6 am but would go straight back asleep again. It worked well as early morning was when he had seizures so we could keep an eye on him.

|

|

|
We finally got a diagnosis for Charlie when he was aged 12 – this was due to another child with NCBRS coming into the hospital. The genetic test was sent away to the same lab that Charlie’s was sent to in 2009 – the other child also had a SMARCA2 deletion, but this time the lab was aware of the connection to the syndrome. They had Charlie's result in their database and made the connection and informed the genetic consultant who informed us. We were happy to have a diagnosis 10 years on and be able to join the NCBRS community for support.
Charlie is now 13 and hitting puberty and has taken a growth spurt. He is also putting on more weight and actually has a big tummy now compared to how skinny he previously was!! His behaviour has gotten a little more aggressive with puberty and he can push people (he is quite strong now) and he uses bad language when he does not get his way. Hoping this will resolve. He normally calms quickly with a short sit on the stairs until he says sorry.
He has delayed eruption of teeth – still has all his baby teeth (bar 2) which are now spacing due to jaw growth. He has an adult tooth coming down with no space for it so will need to go back to the dentist.
Charlie, I would say is the heart and soul of the family. He has 3 siblings, but takes over the conversation at most mealtimes. The future is uncertain. His neurologist says he will always be 50% behind the norm, but he does learn and retains what he learns. He has no limits set on him, nor do we set difficult expectations, we take him as the lovable, funny, sociable boy that he is.
Charlie is now 13 and hitting puberty and has taken a growth spurt. He is also putting on more weight and actually has a big tummy now compared to how skinny he previously was!! His behaviour has gotten a little more aggressive with puberty and he can push people (he is quite strong now) and he uses bad language when he does not get his way. Hoping this will resolve. He normally calms quickly with a short sit on the stairs until he says sorry.
He has delayed eruption of teeth – still has all his baby teeth (bar 2) which are now spacing due to jaw growth. He has an adult tooth coming down with no space for it so will need to go back to the dentist.
Charlie, I would say is the heart and soul of the family. He has 3 siblings, but takes over the conversation at most mealtimes. The future is uncertain. His neurologist says he will always be 50% behind the norm, but he does learn and retains what he learns. He has no limits set on him, nor do we set difficult expectations, we take him as the lovable, funny, sociable boy that he is.

|

|
Contact US
|
NCBRS Worldwide Foundation
124 City Road, London, EC1V 2NX, United Kingdom |
|
Vertical Divider
|

|
Home | About NCBRS | What is NCBRS? | Resources for the Newly Diagnosed | Research | Patient Registry | Stories | Resources | Gallery | Events | Store | Donate | Get Involved | Translate
Copyright © 2023 NCBRS Worldwide Foundation | Registered charity in England & Wales 1190194
